
News 1/15/09
From Musing: “Re: EMR economic incentives. Let’s say I am convinced that Congress and Obama will get their acts together and come up with some kind of economic stimulus package that includes an HIT component. If I am a doctor, why would I want to spend my dollars today if Uncle Sam might be willing to help with at least a portion of it a few months down the line?” Quite the conundrum, but you will probably find out soon one way or the other.
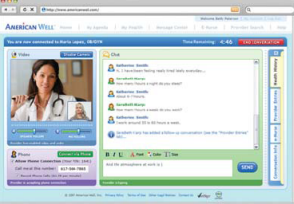
A patient sues her doctor for failing to provide a sign language interpreter for her office visits and wins a $400,000 settlement. In light of that, a provider of American sign language relay services decides it’s a great time to announce its LifeLinks package, which provides remote translation services. To use the service, the practice sets up a computer with a webcam. When needed, the physician and patient receive face-to-face video access to interpreters and sign language specialists. Clients pay only for the specialists’ time.
A physician shares details of how an employee embezzled $50,000 from her over a three-year period. I’m always amazed how often this occurs. The stories always seem similar: the doctor is consciously providing the best quality care in a busy practice and defers all business activity to a trusted employee. If someone is determined and greedy, they’ll figure out a way to outsmart even the best computer system.
A Canadian woman files suit against Purdue Pharma for $31 million, claiming she became addicted to their drug OxyContin. She’s applied for certification as a class action on behalf of all OxyContin users in British Columbia.
Economic conditions lead to an increase in bartering goods for medical services. A couple of Maryland doctors have been bartering with patients since opening their practice three years ago and believe it has helped grow their business. Typical exchange items include office supplies, staff meals, plumbing work, and other goods and services.

AAFP President and family practice physician Ted Epperly is a fan of electronic medical records. "I’m a big proponent. We’ve had an EHR in our practice here in Boise for four years. It’s revolutionized my practice. I’m more efficient. I make fewer errors. My data are more retrievable. I can give feedback to both my practice and that of my colleagues and the residents I’m fortunate enough to be able to train."
To your right: enter your e-mail address in the Get Instant Updates box to be the first to know when we write something new. Just below that, click the Email This to a Friend graphic to recommend HIStalkPractice to friends and colleagues (thank you!) And, a little further down, you can search both HIStalkPractice and HIStalk in one easy Google box, finding out whether we’ve ever mentioned you.
Is EMR not the silver bullet after all? Booz Allen Hamilton and the Federation of American Hospitals release a report that concludes HIT emphasis needs to be on improving electronic communication among patients and providers rather than getting EMRs installed. Among other key points, the report recommends focus should be on e-Rx, electronic results, and medical imaging. Also, payments should tie to desired outcomes. In addition, patients need access to their records and have a way to communicate with their physician about them.
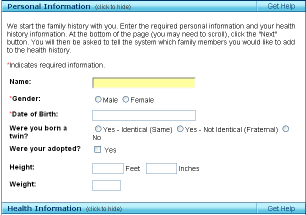
HHS announces rollout of an improved version of the Surgeon General’s family health history Internet site called My Family Health Portrait. It was built to follow data exchange standards that will allow it to exchange information with practice EMRs.

A Las Vegas physician who planned to retire soon is shot dead in her medical office exam room by an 80-year-old patient who then killed himself. Police have not determined a motive.
The ambulatory care sector adds 14,000 jobs in December, despite the country’s overall loss of 2 million jobs. Hospitals added 12,000 positions and long-term care/home-health grew by 2,000.
The State of California investigates Kaiser Permanente and the protocols it uses in its call centers. The investigation stems from complaints of mishandled calls that compromise patient care. The state wants copies of the call scripts that Kaiser’s unlicensed staffers use to make medical decisions. Kaiser claims the scripts are proprietary.
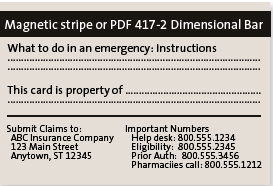
City employees in Warwick, RI receive free enrollment in a PHR program that gathers basic health information into one secure place and releases it to appropriate healthcare providers. The ER Card is developed and controlled by the individual, containing only the information they choose to enter. The patient is responsible for keeping it up to date and the record will not include doctors’ notes. The city seems pretty proud of this great new employee benefit. Perhaps they haven’t heard of the little company in Redmond, WA that offers a similar free service via the Internet.
The doctors at Johns Hopkins University’s Wilmer Eye Institute know all about HealthVault, since HealthVault’s Be Well Fund is underwriting their automated patient reminder trial. Wilmer Eye will use MEMOTEXT to send glaucoma patients customized reminders via e-mail, text message, or phone call, reminding them to take their medications. The trial is designed to measure if automated reminders improve adherence to prescribed medication regimes.

President Bush’s physician, like several other members of his administration, gets a last-minute obscure government job, appointed to finish a term on the US Air Force Academy’s Board of Visitors.
Staff working the ED at Waseca Medical Center (MN) wear white coats and stethoscopes, but they aren’t doctors. The hospital interprets state regulations requiring physician assistants and nurse practitioners to be supervised by a physician as meaning it’s OK to have that doctor available by telephone if needed. A 2007 survey said that one in seven rural hospitals staffed their EDs entirely with PAs and NPs.
Incoming HHS Secretary-designate Tom Dashchle wants Congress to shift the nation’s healthcare model to emphasize wellness and prevention by providing more support for primary care doctors. "Every country starts at the base of the pyramid with primary care and works their way up until the money runs out. But the United States starts at the top of the pyramid and works its way down until the money runs out, resulting in a lack of primary care and wellness."
Ben Brown with KLAS Research claims that healthcare’s speech recognition market is on the verge of a "long-term growth curve of adoption.” Brown predicts adoption rates will continue to climb because speech recognition provides a “clear” ROI. Also, look for it to be increasingly integrated with EMRs.
The Agency for Healthcare Research and Quality launches a Web site that advises clinicians and consumers on emerging drug therapies. The site also provides access to education and information resources designed to improve healthcare quality, safety, and effectiveness.
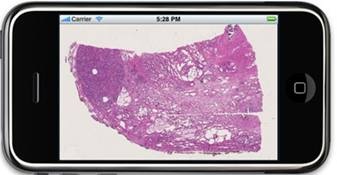
Here’s a cool new iPhone application for the pathologist on the run. The Institute for Medical Informatics, Rikshospitalet, Oslo University Hospital develops a remote application for the review of pathology images on the Apple iPhone.
The Duke Endowment awards $99,000 to Caswell Family Medical Center for the purchase of an EMR. Caswell Family is a five-provider practice in North Carolina.
Former MedComSoft VP Mary Torrance joins Electronic Healthcare Systems to serve as EHR consultant for the CareRevolution product.
Telephone equipment maker Nortel Networks files for Chapter 11 bankruptcy protection .






The article about Pediatric Associates in CA has a nugget with a potentially outsized impact: the implication that VFC vaccines…